Inside the murky, high-stakes investigation into New Brunswick’s mystery illness
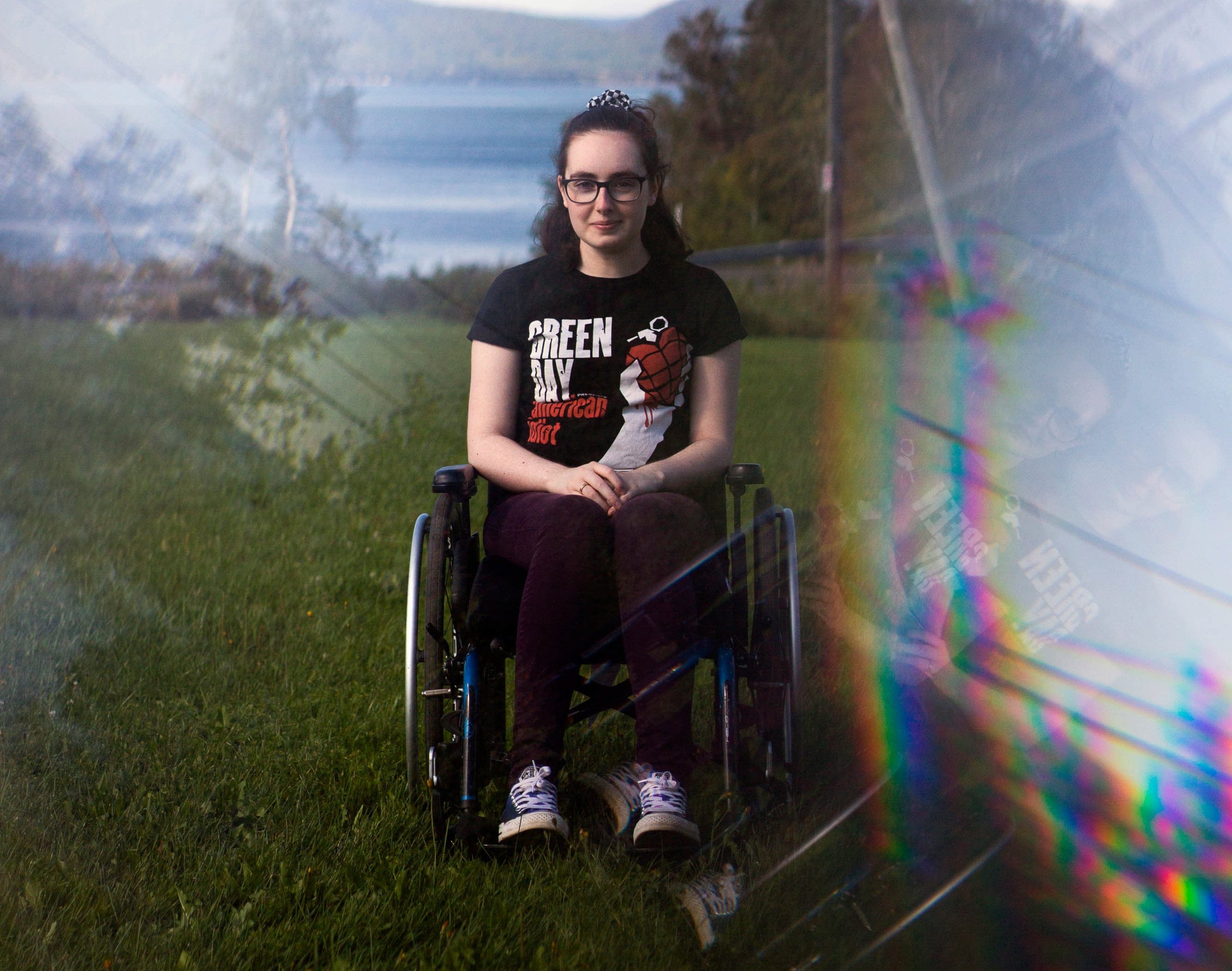
On a Sunday night in late October 2019, Gabrielle Cormier set her alarm and fell into a deep sleep. The first-year student at Mount Allison University woke to someone knocking on the door of her dorm room. Confused, she pulled out her phone and saw the time: 5:30 p.m. Cormier had slept 20 hours—through the night and the following day, missing every one of her classes.
Cormier stumbled out of bed, groggy and unbalanced. When she opened the door, a friend stood on the other side. He asked if she wanted to get something to eat. Cormier fumbled for words in response. Her actions seemed so odd that he took her to the hospital instead.
There were no answers for Cormier that day or the days after. Even now, no one knows what is happening to her, what caused it or how to fix it.
Something is wrong with Cormier’s brain. She forgets things and becomes easily confused. She watches the same television shows on repeat because she can’t retain new information. She’s losing control of her muscles. The girl who used to be able to dance en pointe needs a cane or a wheelchair to travel any distance. Her long dark hair goes unwashed because her arms are too weak to clean it.
Cormier, 20, is one of 48 people in New Brunswick who are part of a cluster of cases of a progressive neurological syndrome with no known cause. At least six people have died. Their ages range from 18 to 85, and most live in the Acadian Peninsula and Moncton areas of the province. They have an unusual mix of symptoms—combinations of anxiety, dizziness, hallucinations, pain, memory problems and progressive loss of mobility.
Related Posts

Why sanctions over the Ukraine invasion won’t stop Putin

‘Anybody want to drive this ambulance to Ukraine?’

For months, the province has been leading an investigation into the cluster. The work is still in the first stage: confirming that, in the midst of the COVID pandemic, people in the province are falling ill with a neurological disorder of unknown cause.
The Public Health Agency of Canada, or PHAC, triggered an alert about a high number of unusual neurological cases in the province late last year. The agency provided specialized expertise early in the investigation by interpreting diagnostic and autopsy results, and worked with a New Brunswick neurologist to establish a case definition for the cluster.
But, over the last three months, PHAC refused multiple requests from Maclean’s to speak with its scientists—including scientists who gave interviews last spring and have since gone silent. PHAC says that the province of New Brunswick is now leading the investigation, and the federal agency’s role is a supportive one.
A federal public servant, who was not authorized to speak on the record, told Maclean’s: “PHAC is no longer in the cluster investigation business.”
Currently, no scientists are performing environmental testing as part of the investigation.
The patient safety organization Blood Watch says it is concerned by the lack of environmental testing. The group wants PHAC to take the lead on the investigation, and is calling on the federal agency to “immediately resume its investigation into the root cause” of the cluster. In a letter addressed to federal Health Minister Patty Hadju and Chief Public Health OfficerDr. Theresa Tam at the end of September, Blood Watch wrote, “families in New Brunswick deserve answers, which are supported by full scientific rigour, as to why their family members have perished and why patients are becoming ill from painful and debilitating neurological diseases.”
“All scientific investigation and research must be free from any political interference,” the organization wrote. “We are asking that you issue a clear directive that the investigation must continue solely through a scientific lens.”
READ: Researchers looking for mRNA were ridiculed by colleagues. Luckily, that didn’t stop them.
Anna Maddison, spokesperson for PHAC, says the province has jurisdiction over the investigation. PHAC “will continue to be ready to support the province as its investigation unfolds, and stands ready to provide additional support, if needed or requested,” she wrote.
Meanwhile, people in the province are sick. Some have died. Many are anxious. No one knows who is at risk or how many are ill or how many could die.
People fear answers will come too late.
***
Cormier grew up in the village of Balmoral, N.B., a francophone community that takes up a narrow stretch of land just south of the province’s northern shore. Her parents divorced when she was eight. She’s close with both of them, as well as with her sibling and step-siblings. As a toddler, she suffered one seizure during a fever; as a teen, she struggled with anxiety, but never had major health issues. She figure skated, skied, danced and acted in school plays. As a kid, she developed a deep devotion to the band Green Day, sparked by the way that her dad would pluck out their hit “Time Of Your Life”for her on his guitar.
Cormier excelled in school, particularly math and science. Growing up, she asked for science kits and anatomy books for Christmas. She set her sights on becoming a doctor—a pathologist, the kind of doctor who specializes in diagnosing disease through body tissues and fluids. She received high marks in school, earning bursaries that covered most of her university tuition.
It’s impossible to pick out the exact moment that whatever is hurting Cormier’s brain began its destructive path. In hindsight, a few odd things stand out to her from her last year of high school. That spring, as she put her books away before drama practice, she passed out. A friend found her on the floor and called an ambulance. At the hospital, says Cormier, a doctor dismissed her episode as a panic attack, even though she told him that she knew what a panic attack felt like—this was not that. She says the physician told her to get off her anxiety medication or she’d struggle at university. A week or so later, she felt a weird tingling in her hands and feet that wouldn’t stop. In ballet, her leg muscles started to shake during moves that once came easily. She saw a doctor again over the summer because her feet and her lower legs were turning “kind of blue.” There was nothing there, she was told.
MORE: The year of the pandemic has busted the myth that Canada values its seniors
In September, she moved to Sackville, N.B., for university. On campus, Cormier grew tired walking from one class to the next and sometimes walked crookedly, bumping into people. Her lack of coordination became a joke among her and her friends. After the day Cormier didn’t wake up for class, doctors tested her for mono. The results came back negative. She hoped that whatever was plaguing her would blow over. On good days, she could still go to class and do assignments but mostly, she skipped school to rest. She lost weight, unable to eat from nausea.
At the end of term, she wrote only three of her five scheduled exams. At the top of one, she scribbled a note to her professor, who’d been kind to her during her hospitalization earlier in the semester. “See you next year,” she wrote, thinking that she’d be back to retake his class the following autumn.
***
The first alert of something being amiss in New Brunswick went out in December 2020, when experts at Canada’s Creutzfeld-Jakob disease (CJD) surveillance system, which is operated by PHAC, notified the province’s chief medical officer of health about an unusually high number of cases of something in the province that looked like CJD but was not.
A quick-moving and fatal neurodegenerative disorder, CJD is the most notorious member of the family of prion diseases. Prions are abnormally folded proteins capable of making normal proteins also misfold. They lack DNA or RNA, so they are not expected to replicate in the way that viruses do. Yet they do propagate and cause damage leading to progressive neurodegenerative diseases that have no cure.
READ: We gave them our leftover frozen embryos. Now, we’re a family.
Overall, CJD is very rare, affecting one to two people per million annually. It can happen because of a genetic predisposition, by chance or from exposure to an infectious form through, for example, a corneal transplant or infected surgical instruments. According to PHAC, 90 per cent of CJD cases in this country occur spontaneously.
Since the 1990s, when a new prion disease—known as variant CJD, or vCJD—spread in the United Kingdom after people ate meat from diseased cattle, health agencies around the world have tracked cases of CJD. In Canada, physicians report anyone with suspected CJD to a national surveillance system. Between 1998 and August 31, 2021, doctors in Canada referred 2,324 cases to the country’s national surveillance program. Once a patient is referred, the CJDSSlab conducts testing to confirm a diagnosis. It’s the only place in the country that can do so. Of the patients referred to Canada’s surveillance system, about half—1,156—have received a definite or probable CJD diagnosis. This includes 37 people from New Brunswick.
The December 2020 alert came after experts at the CJD surveillance system noticed a jump in cases of suspected CJD from New Brunswick: 12 cases in 2019, another 29 in 2020. The trend continued into 2021 with another 24 in the first seven months of the year. Tests ruled out CJD in the vast majority of cases, but the scientists at the CJD surveillance system decided that an unusual pattern among some of these referrals warranted investigation.
In March 2021, as Canada’s third wave of COVID-19 began its wicked climb, New Brunswick’s chief medical officer of health sent an internal memo to doctors and nurses, alerting them to a cluster of 42 patients with a neurological syndrome of unknown cause. The patients mostly lived in the eastern part of the province. Since then, the cluster under investigation has grown to 48 cases and six deaths.
The province’s memo described people in the cluster as having becomesick with rapidly progressing dementia, along with issues with gait and muscle coordination, memory loss and brain atrophy that was worse than expected for their age. Doctors were asked to be on the watch for patients with these symptoms and no obvious diagnosis.
Within days, Radio-Canada received a leaked copy of the memo. The story made headlines around the world. People reached out to Canadian neurologists, worrying that they, too, had this condition, or that a family member did.On the other side of the country, the inbox of Valerie Sim, an associate professor of neurology at the University of Alberta and expert on prion disease, lit up with messages. “I’m getting emails from people all over the world saying, ‘Oh, I have this,’” she told Maclean’s in July.
READ: How do I get my vaccine passport? Where will I need to show it?
Sim says it’s not clear to her that patients in the cluster are suffering from a single syndrome. She has not seen data on patients, but has read public reports and talked to experts familiar with the investigations conducted by the CJD surveillance system. “I’m not in any way trying to say that there isn’t a syndrome. I’m not trying to say that they couldn’t all be the same,” she says. “I’m just putting it out there that there’s no reason we have to think that this is anything.”
Sim says health care providers and scientists have a responsibility to communicate with the public and not hide information. Instead, she says, the way the story became public “has caused harm, where perhaps there’s not even a story.”
***
Gabrielle Cormier went home at Christmas in 2019 and her family physician referred her to a neurologist in Moncton, Dr. Alier Marrero. As Marrero checked Cormier’s blood pressure on that first visit, her leg jerked involuntarily. He asked if that happened often; she realized it did.
Cormier returned to Mount Allison after Christmas, but she felt worse. In February, she quit university. Later that month, as she underwent her first spinal tap, she told Marrero that she’d dropped out of school. It was probably a good idea for the time being, she remembers him telling her. Sometime over the next year, she says he told her that there were other patients similar to her.
Born in Cuba, Marrero completed his neurology training in Quebec before settling in New Brunswick in 2013. He has a longstanding interest in neurodegenerative diseases like amyotrophic lateral sclerosis, or A.L.S., and rare diseases. Both Quebec and New Brunswick are good places to study rare conditions.Many residents descend from French settlers who colonized Quebec and the Acadian Peninsula beginning in the 1600s. Founder mutations—genetic alterations that emerge in geographically or culturally isolated populations—have been identified in these areas. Sometimes founder mutations are linked to rare diseases, including neurological ones. For instance, in the 1970s, a neurodegenerative disorder known as ARSACS was first described in 200 families in the Saguenay-Lac-St-Jean area of northeastern Quebec. Its name—short for autosomal recessive spastic ataxia of Charlevoix-Saguenay—reflects the region where it was discovered and where incidence is higher than the rest of the world.

In the past, Marrero and colleagues have identified genetic conditions stemming from unique mutations among the population of New Brunswick. They’ve published three case reports and have several more not yet published, Marrero says. Because of this kind of work, he often receives referrals of patients with unusual neurologic symptoms—including many over the last three years whose condition made him think of CJD. The patients had neurodegenerative symptoms, often quickly progressing; but despite the usual work-ups, he had no diagnosis for them.
Neurodegenerative diseases, like CJD, remain a mystery in the scientific world, Marrero says. “This is a territory where we have a lot to do in general in science because neurodegeneration [causes] the diseases of our time,” including dementias and Alzheimer’s disease, he says. “We don’t have a cure for any one of them.”
Marrero reported his patients to the federal surveillance system for CJD; their symptoms were similar to CJD or vCJD. The province says 46 of the 48 patients in the cluster currently under investigation in New Brunswickwere reported by Marrero, and a 47th was co-reported by Marrero and another physician. (Maclean’s interviewed Marrero by phone in early July; when Maclean’s contacted Marrero in late Septemberto confirm these numbers, he said he was required to refer all media requests to the province.)
MORE: Canadians died of drug poisoning every 49 minutes during one dreadful week last summer
Many of the patients experience a similar pattern of symptoms, Marrero says. First, they have mood and behavioural changes, along with sleep disorders. They become very anxious, maybe for the first time in their lives. Some have hallucinations or terrifying dreams. A few have delusions where they think their loved ones have been replaced by imposters. They lose the words for things or people they know. Some have echolalia, a condition in which a personrepeats the same word or sentence. Those who are high-performing can cover up changes early in their disease, but they eventually make mistakes at work or school, says Marrero. Many develop blurry vision and dizziness. Nearly all the patients in the cluster have myoclonus, involuntary muscle jerks. They have pain in their arms and legs, and lose weight rapidly. As they worsen, they lose motor skills and functional capacities, but they deteriorate at different speeds. Patients have had CT scans, MRIs and blood work, and many have had genetic testing. Some have received therapies like intravenous immunoglobulin, steroids and medications for Parkinson’s and epilepsy, but unsuccessfully.

Marrerohas seen some cases within families but does not believe this is a genetic syndrome. There are cases of “biologically unrelated” patients who live together and have similar symptoms.
As word spread about the cluster, Steve Ellis thought the patients sounded like his dad. Roger Ellis, a 63-year-old retired industrial mechanic who spent his career working in mines, went to the hospital one summer weekend in 2019* as he and his wife werecelebrating their 40th wedding anniversary. Roger worried that he was having a heart attack. He underwent tests and was sent home, twice. But on Sunday evening, Roger began vomiting and passed out with a seizure. Ellis’s sister called an ambulance. At the hospital, their father’s seizures eventually improved, but other symptoms emerged. Doctors ruled out epilepsy, CJD, autoimmune encephalitis, exposure to lead, rare cancers and brain tumours, Ellis says. But Roger, who had been the caregiver for his wife, did not recover, despite a variety of treatments. He spent 366 days in hospital before being moved to a care home. Roger, who has been a patient of Marrero’s since April 2021, struggles with speech, memory and hallucinations. His son says he shuffles rather than walks and has lost his mechanic’s dexterity. “It’s been horrible to watch. He’s changed in every single way,” says Ellis.
Ellis set out to find some of the families in the cluster, looking for people who might understand what his family was going through. He created a Facebook group, which has grown to more than 400 individuals. Some joined because they worry that they or someone they care for might have this condition; many are from outside New Brunswick. Only a handful of people, including Cormier, have come forward as part of the cluster.
Ellis was shocked when he learned how young she was.
“That’s the thing that I’m so puzzled about,” he says. “What is this that can get two people so far apart in age so sick?”
***
In May, the province’s public health experts began interviewing people in the cluster as part of an epidemiologic investigation, asking patients and their families about things like their environment, homes, eating habits, past illnesses and travel, using a questionnaire developed in collaboration with PHAC. By the end of July, 23 patients had been surveyed, Cormier and Roger Ellis among them.
READ: Typical ’vaccine hesitant’ person is a 42-year-old woman who votes Liberal: Abacus polling
The results of these questionnaires are currently being analyzed, according to the province.
Édouard Hendriks is co-chair of the province’s committee of six neurologists who are now overseeing the investigation. Their first step is to confirm that no one in the cluster has a missed diagnosis, a known condition—like Lewy body dementia, a progressive dementia associated with abnormal deposits of the protein alpha-synuclein in the brain—that could explain their sickness. Hendriks says he expects some patients will be found to have known conditions and be removed from the cluster. But all other possibilities, including a novel prion disease, are “still on the table,” he says.
In July, New Brunswick Health Minister Dorothy Shephard told Maclean’s that she expectedthere would be no answers for at least four to six months. “The most important thing to know is that not only have we not ruled anything out, but we haven’t ruled anything in,” she said.
PHAC’s involvement is currently focused on investigating and ruling out CJD, the province confirmed. “As there are no cases reported by other neurologists or health care providers from other provinces or territories within the identified cluster of cases, the investigation is a provincial matter currently,” Bruce Macfarlane, a spokesperson for New Brunswick department of health, told Maclean’s by email in early October. “However, as with any situation where public health risks are identified, it is common practice for our provincial public health officials to collaborate with PHAC colleagues.”
READ: The unsettling case of Dr. Ngola, the RCMP and the New Brunswick government
Neil Cashman, a professor of neurology at UBC who is an adviser to PHAC and the CJD surveillance system, says he offered to provide on-the-ground support in New Brunswick but was turned down by the province. He says he is pleased that the province is taking the first steps to verify whether an outbreak of something unusual is happening. Buthe wants outside scientists involved who can begin investigations into possible environmental factors that could be causing a flare of neurodegenerative illnesses in New Brunswick.
“I can see the value in starting at square one. I also worry that we need to get started on this research ASAP,” he says.
Cashman says he believes that this syndrome could be caused by exposure to BMAA, or β-methylamine-L-alanine, a neurotoxic non-protein amino acid. After the American capture of Guam in 1944, a neurologist with the U.S. Navy noticed extremely high rates of an ALS-like syndrome among the island’s indigenous Chamorro people. The Chamorro even had a word for it: lytico-bodig. By the 1950s, ALS incidence was 100 times higher in Guam than elsewhere in the world. There were other presentations of the syndrome, too, in people with symptoms similar to Parkinson’s and dementia.
Early on, researchers tied the syndrome to the cycad plant, which islanders ground up for flour when imports were restricted during World War Two. But it took another two decades of research to isolate BMAA as a possible cause. BMAA is in the cycad plant and also in cyanobacteria, blue-green algae. BMAA concentrates as it moves up the food chain, accumulating in some seeds, bats, shellfish, lobsters and other marine seafoods.
MORE: These adventurers are on a 7,600-km journey from the top to the bottom of Canada
In humans, some studies have suggested BMAA is correlated with different kinds of neurological disorders, though the association remains controversial. There is no definitive study showing that BMAA causes neurological disease in humans.
If BMAA is linked to the illnesses in New Brunswick, a great deal of testing and science will have to be carried out to confirm the connection, says Cashman. “But as I say, at this point, we don’t have the go-ahead on this sort of scientific program.”
Paul Cox, an ethnobotanist at the Brain Chemistry Lab in Jackson Hole, Wyo., who spent years studying the people of Guam, says it isn’t clear to him that any environmental toxin is at play in New Brunswick. Still, Cox says chronic exposure to BMAA could possibly trigger certain types of progressive neurodegenerative illness, as could many other toxins that cyanobacterial blooms produce. As the climate changes, algae and cyanobacteria bloom more often and in larger size—meaning people are more likely to be exposed, he says. “We believe BMAA is a trigger in susceptible individuals for certain neurodegenerative diseases. So just living near it does increase your risk,” he says.
If BMAA or other environmental toxins were to be investigated as a potential cause, detailed epidemiological investigations would need to be carried out, Cox says,along with regular sampling of cyanobacterial scum over time and lab tests on tissues from people who’ve died with this syndrome. “There’d be no problem with fielding a dream team that could do that in Canada,” says Cox.
READ: Clinic 554 for sale as N.B. government refuses to cover cost of abortions outside hospitals
Susan Murch, a professor of chemistry at the University of British Columbia, is one of Canada’s leading experts on BMAA. She says BMAA could be a factor in New Brunswick, but other environmental toxins could also be affecting neurological illnesses in the area. “So I think it’s important to start analyzing some tissues from the ecosystem,” she says. “What we do know about New Brunswick is that they are having concurrently both an unusual cyanobacterial bloom and an outbreak of neurological illness at the same time. That’s very unusual.”
Blue-green algae is spreading in New Brunswick, appearing for the first time this year in some lakes and rivers and reappearing in others, according to a CBC report in August. New Brunswick’s Public Health department publishes reports of blue-green algae on its website, including health department advisories.

Murch said that during her research in Guam, she heard from the Chamorro people that they were tired of being treated as test subjects without receiving any answers to what was making them ill. She hopes Canadian scientists, governments and journalists show respect to people who are suffering in the midst of uncertainty. “Be kind to these patients. Having an illness that isn’t well understood is a terrible thing,” she says.
There have been deadly environmental toxins in Atlantic Canada before. In November 1987, government agencies in New Brunswick and Quebec received reports of three people who developed sudden confusion, disorientation and memory loss, along with gastrointestinal symptoms, within 24 hours of eating mussels. Although scientists could not immediately isolate the toxin, Health and Welfare Canada issued a warning to avoid eating mussels from Prince Edward Island and shipments from the island were temporarily halted. Within two weeks, scientists identified a cause: domoic acid, a potent excitatory neurotransmitter, which grew from an extensive algae bloom in eastern Prince Edward Island in November and December 1987, and disappeared soon after.
READ: The search for graves—and truth—at a Nova Scotia residential school
By the time the investigation was completed, more than 100 people became acutely ill from the outbreak, four of whom died.
Michael Strong, a neurologist and president of the Canadian Institutes of Health Research, says it will take time to find an answer to what is happening in New Brunswick. “I would say, definitively, you’re not going to have an answer in four to five months,” says Strong. He noted that an interesting challenge in New Brunswick is that the illness looks like diseases seen before, but not exactly. “And so is it something that’s new?” Strongsays.
Marrero believes what is happening in New Brunswick is something acquired through the environment, although he does not have any evidence as to what. He thinks the yet-inexplicable neurological changes in his patients are an indication that people are not adapting as quickly as the climate is changing. “I do see our condition as a canary in the coal mine,” he says.
He believes that this syndrome is affecting people outside of New Brunswick, pointing out the province’s proximity to Quebec, Nova Scotia, PEI and the state of Maine. “We’re surrounded by the same ocean, the same kind of weather and climate and everything,” he says.
Although the investigation is centered on the 48 people in the cluster, more have reported symptoms.More than 80 people have been seen at Marrero’s clinic since this spring.
***
At the heart of this mystery are people who are very sick or have died, and their families. They are afraid and desperate for answers. Ellis wants more information from the provincial government. “I believe they’re hiding something,” he says.
The New Brunswick Public Health department is “committed to sharing the findings of this investigation to patients and their families as well as the public as soon as they become available,” Macfarlane told Maclean’s.
The department of health has not provided any details on the six people in the cluster who died, nor acknowledged any others who may have died. Ellis and Blood Watch saythe department has refused to release the copies of the epidemiologic interviews to the families; the province told Maclean’s that copies of interviews and personal health information cannot be shared for privacy reasons, but a summary report will be shared with the public as soon as the analysis is complete.
The province hasnot released information on where people in the cluster are located. Most of the people under investigation were living in the southeastern and northeastern regions of the province when they were referred. Macfarlane told Maclean’s that, “so far, our investigation has not found any evidence suggesting that the residents of these regions are more at risk than those living elsewhere in the province.”
MORE: When you can’t trust what you see: Life with a perception disorder
In July, Shephard, N.B.’s minister of health, said some patients had moved; she said she wasconcerned that the ongoing investigation could be biased if those geographic details werereleased to the public.
The province has not released information on the results of autopsies that were completed. Autopsy reports are considered personal health information and their results cannot be shared, said Macfarlane,but the findings will be summarized in the final report.
In an email to Maclean’s,PHAC confirmed that five autopsies have been completed through the CJD surveillance system and that these showed no evidence of prion disease. The province’s oversight committee has met with the pathologist to review the autopsy findings, said N.B. spokesperson Macfarlane.
Three individuals familiar with the investigations told Maclean’sthe autopsies revealed no unifying pathology among the patients. Instead, these individuals suffered from varying disease processes before they died, said sources.
But those results do not rule out the possibility that an environmental trigger is causing neurodegenerative illnesses in these patients, says Kat Lanteigne, co-founder of Blood Watch. The organization wants a team of PHAC investigators on the ground in New Brunswick and a patient representative on the investigation team. They want testing performed for BMAA, given the blue-green algae presence in some of the province’s watersheds, she says.
“What the federal scientists bring to the table is not only world renowned expertise…but it also commands a level of transparency,” says Lanteigne. “That is so critical when you’re dealing with an emerging public health crisis, which is what this is.”
Shephard, the health minister, said she understoodpeople’s anxiety, but thatno one wants the province to jump to conclusions. “We have committed to doing this research and reviewing the information in a very quick manner, four to six months,” she said. “We’re doing that because we want to give New Brunswickers peace of mind. And hopefully that’s what we get at the end of this.”
The province did not rule out BMAA testing as part of the investigation: “Once the investigation is completed and potential causes and risks are identified, we will follow up as appropriate,” said Macfarlane.
In early October, Maclean’s asked the province when they planned to share any findings or next steps with the public. Macfarlane said that “results of the epidemiological investigation will be shared as soon as they become available. Further clinical findings will be shared once the investigation is completed.”
***
In the meantime, patients are getting sicker. They show up at their appointments, full of questions that don’t have answers. Marrero says he sometimes pauses between visits with patients. He meditates or tries to focus on something else. He reminds himself that he must start from zero with every person, that their story is not the same as that of the last, that every person in the cluster needs their own answer. “I am hoping for these patients to find something, and I’m really working for that,” he says.
Cormier still sees Marrero, as well as a psychologist and physiotherapist. She misses her friends who are now in their third** year of university. They video-called her over the summer as they played board games. She laughed during the call, but wept after it ended. She’s tired of being home alone; she dreams of seeing Green Day in concert and doing the kinds of carefree things that people her age are supposed to get to do. She doesn’t know if she’ll get a chance.
“I have faith in Dr. Marrero. But I am a realist. And there’s a very real possibility that I’ll never get better or not survive this,” she says. “I am hopeful that the third option, which is getting better, happens.” The third option is heavy with dreams, including travel, concerts and a career in pathology.
*A previous version of this story reported that Roger Ellis first went to the hospital in 2020. In fact, it was in 2019.
**A previous version of this reported that Gabrielle Cormier’s friends are now in their second year of university. In fact, they are in their third year.
Related Posts

“Sixty-three per cent of N.W.T’s population have been evacuated”

The case for an inquiry into Canada’s treatment of First Nations children

The Power List

Why Hamilton is now permitting homeless encampments and tiny homes in parks
Get the Best of Maclean’s straight to your inbox.
Sign up for news, commentary and analysis. Join 60,000+ Canadian readers.