
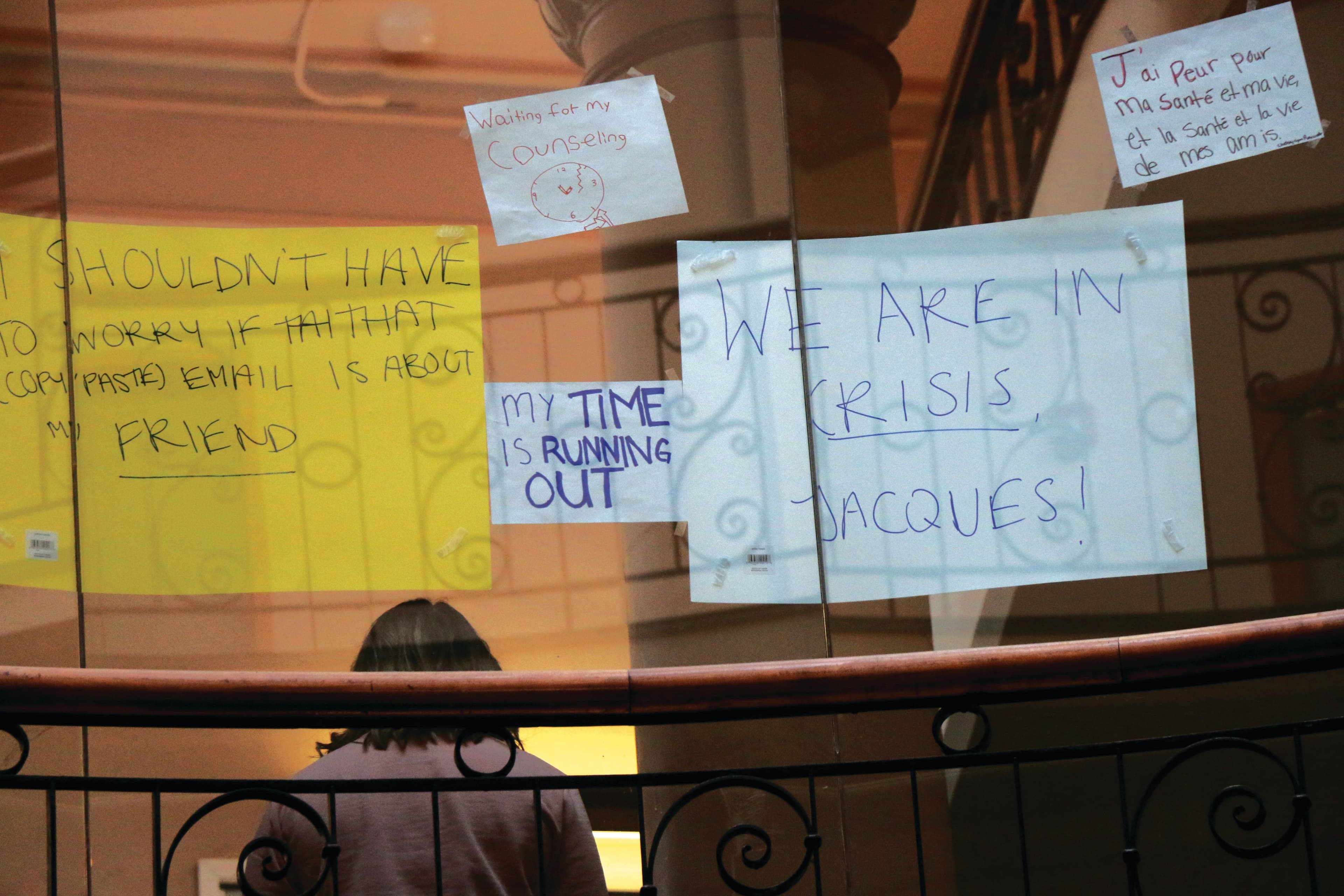
Inside the mental health crisis at Canadian universities
Before the pandemic descended and emptied its hallways, the Davis Building at the University of Toronto’s suburban Mississauga campus (UTM) was a busy hub of academic and social life, and the students walked with a briskness that matched the pace in any urban rail station. The campus’s Health and Counselling Centre (HCC) is just down a set of stairs, in the basement of the building. Last November, a young woman went there after struggling with feelings of being overwhelmed and anxious about living up to academic demands and grappling with unresolved trauma. Anushka* was experiencing suicidal ideation that culminated in a specific plan involving a bottle of pills that she carried in her backpack.
Anushka says that after seeing a nurse and a doctor, she was told she would need to be admitted to a nearby hospital. Anushka asked if she could go to the hospital the following day, after a big test she had been preparing for. The doctor said it had to be that day, says Anuskha. “I asked if I could go to my lecture because the test was going to be based on the lecture. She said no, that I was going to have to go now and that she was going to have to call the campus police.” Anushka asked if a friend could come with her to the hospital and the doctor agreed. When Peel Police arrived, Anushka says, they told her that she was being taken into custody. They told her that her friend, who had by now arrived at the HCC, could not come with her. Anushka began to panic and then cry, as her fear and confusion mounted. According to Anushka, the police marched her to a police car parked behind the busy central bus stop, and the officers told her they would have to put handcuffs on her before placing her in the car. She pleaded that it was unnecessary, now crying harder, but they insisted. Anushka says the police took her to the Credit Valley Hospital in Mississauga, Ont., where she saw a psychiatrist who told her to keep seeing a counsellor and then sent her home with a medical note.
[contextly_sidebar id="pNngi81Zs5d94Y4mJEBZLBli9G34nP79"]
Anushka told me her story in January while sitting in a Starbucks, just a short drive from UTM. She was immaculately dressed, with perfectly applied eyeliner and long, thick black hair that she kept tucking behind one ear. But the depth of her fragility in that moment was plain, and her voice wavered as she described her experience—and how it deterred her from seeking further help.
When I asked the University of Toronto whether the school has a policy of requiring students to speak to the police when they have expressed suicidal intent and are willing to go to the hospital, a university spokesperson provided the following statement: “Students who seek help are cared for by medical professionals trained to work with individuals experiencing a mental health crisis. Hospitalizations are relatively rare, and most are voluntary. Campus police become involved only when an individual makes specific statements that indicate they have an intention to do harm such as suicide and are unwilling to go to the hospital. While there is no specific policy in such cases, we have a responsibility to keep individuals safe.”
Related Posts

I Let an AI Avatar Teach My University Course

Canada’s Best Universities in 2025 by Student/Faculty Ratio
The University of Toronto did not respond to specific questions about this and other reported handcuffing incidents on campus, except to note that campus police are reviewing their policies on the use of handcuffs. Const. Bancroft Wright, a spokesperson for the Peel Regional Police, provided a written statement, noting that handcuffing is used “to prevent a person’s escape, for the member’s safety and for the subject’s safety. The use of handcuffs is mandatory on all persons taken into custody, unless in the member’s judgment, the circumstances make it impossible or unnecessary (e.g., children, elderly or physically challenged prisoners).”
In December, U of T released a 24-page report by the Presidential & Provostial Task Force on Student Mental Health that offers an overview of existing services and makes recommendations for moving forward—including the creation of a “culture of caring.” The report also recommended that “a trauma-informed protocol to support campus police in their evaluation of the safety and risk of students transported to the hospital for further assessment be developed.”
Students who were handcuffed while seeking out care have not received the apology they hoped for. Natalia Espinosa, who went public with her own experience of being handcuffed by campus police last November, says it has been hard to get clear answers about any changes to the school’s policy. “I was told that the process was necessary for my own safety, but I didn’t feel more safe,” she says. “I wanted the help and I would have gone willingly. It’s extremely stigmatizing and criminalizing. Students should not be punished for seeking out help.”
***
These concerns are not unique to U of T. Anushka and Natalia’s stories underscore a critical and ongoing crisis at Canadian universities: the vulnerability of students seeking out care, and the problems and limitations with institutions’ responses. They also reflect a broader crisis in youth mental health across Canada, which has seen increasing rates of depression, anxiety and suicide among young people over the past decade.
From 2007 to 2017, emergency visits related to mental health concerns for Canadians aged five to 24 increased by 75 per cent. According to the Centre for Addiction and Mental Health (CAMH), 70 per cent of mental health problems have their onset during childhood or adolescence, young people aged 15-24 are more likely to experience mental illness and/or substance abuse disorders than any other age group, and 34 per cent of Ontario high school students indicate moderate to serious psychological distress, including symptoms of anxiety and depression. “Young people are telling us quite directly that they are feeling really anxious and overwhelmed, that they’re struggling with mood issues and they’re looking for support,” says Joanna Henderson, a psychologist with CAMH who specializes in child and youth mental health.
The pandemic is only making things worse. In addition to generalized fear and anxiety, students have had to adjust to mostly remote learning and the potential severance of their support networks. Part-time jobs may have been lost, parents might be facing unemployment and making rent might seem impossible. On top of that, the commitment to post-secondary education is largely predicated upon preparation for a desirable future, but that future feels particularly cloudy and uncertain at the moment, and some students might be wondering if they will ever have the chance to apply what they’re trying to learn.
But Henderson says the pandemic itself is not the main problem for young people, though many are concerned about a family member becoming ill. “It’s the strategies we’re using to combat the pandemic that can result in social isolation and disconnection from the developmental tasks that they have,” she says. “Engaging with education, engaging with friends, romantic relationships, and managing things more autonomously.”
Concerns among post-secondary students across Canada have been fairly consistent: lengthy wait times to see a counsellor, even in crisis situations; inadequate student representation in decision-making related to mental health services; mandated leave policies, which can force an academic leave on students who may potentially self-harm; mandatory sick notes for missed assignments or exams, which place an additional burden on students who are struggling; and overall inaccessible, disparate, opaque, discriminatory and inadequate campus supports.
Universities have argued that they are not equipped to solve these problems. “The need is great and we know we cannot do this alone,” says Sandy Welsh, vice-provost, students, at the University of Toronto, in an emailed statement. “Mental health, and especially providing the treatment needed in complex cases, is primarily the responsibility of the Ontario public health-care system.” A February editorial in the Queen’s Journal, a student-run newspaper at Queen’s University, called for province-wide supports to ensure that students “no longer have to factor available mental health services into their decisions when choosing where they are going to study.”
This October, the Mental Health Commission of Canada (MHCC) is launching a Post-Secondary Students Standard, a set of evidence-based, voluntary guidelines formulated in consultation with 7,500 stakeholders. The standard aims to increase access to student supports, promote resilience in daily life and provide safe institutional environments. “The standard is based on the firm belief that post-secondary institutions can be change agents on mental health,” says Ed Mantler, vice-president, programs and priorities, at the MHCC. “The goal is to provide a consistent, evidence-based framework on which each school can build initiatives that continuously address and improve the mental health of students.”
Alongside high-level efforts to guide universities’ responses to students, students themselves are agitating for change. A rally was held at the University of Alberta in March 2019 after a student who attempted suicide was evicted from campus housing. In February, students at the University of Ottawa staged a protest in front of the president’s office to demand enhanced mental health support after multiple campus suicides. And an online forum in July at Dalhousie University—“Speak Truth to Power: Racism, Mental Health & Healing”—brought together students, faculty and members of the greater community to discuss the heavy toll of racism on mental health both on campus and off.
And so, nudged along by dedicated student advocates, post-secondary institutions are starting to make some positive changes when supports are even more desperately needed.
***
Concerns about access to mental health resources—and about inadequate funding for those resources—are a national, not university-specific, problem. According to CAMH, mental illness in Ontario alone is underfunded by about $1.5 billion. And research by the MHCC found that approximately 80 per cent of psychology care in Canada takes place in the private system.
Joshua Bowman, who was president of the University of Toronto student union at St. George campus for the 2019-20 academic year, says that access to mental health services was the number one concern of his constituency and that students often feel like they don’t have a voice in most decision-making.
“For a lot of students, this is the first time they’re living on their own or even coming to terms with their own mental health concerns,” says Bowman. “The university is in a unique position to cushion that blow. But there’s no explanation for how to interact with health and wellness. Once you get [to the health centre], you’re asked if it’s an emergency. But when you’re standing in a lobby with a bunch of other students who are crying, you feel like you’re taking up a spot. So you say it’s not that much of an emergency, and they tell you to come back.”
In response to concerns about opacity, U of T’s Welsh says the school is partnering with CAMH to overhaul services on campus, including the creation of a single system for all three campuses.
Meanwhile, students are starting to organize, forming groups to support each other and demand change. In December, after the fourth student suicide in a year, a small group of students at the University of Ottawa formed the uO Collective 4 Mental Health. The group launched a petition demanding a roundtable with all stakeholders, the hiring of more front-line mental health personnel, training on mental health for staff and faculty, clarity surrounding internal and external mental health resources, and the alleviation of out-of-pocket costs for private counselling and pharmacare. The petition garnered over 8,200 signatures. In August, uO Collective and another student advocacy group, U of T Mental Health Policy Council, co-hosted a summit on student mental health that included a discussion of “best practices for creating systems-level change in Ontario.”
“The programs offered [at U of O] are very ineffective,” says Tausif Ahmed, a third-year health sciences student and executive member of the uO Collective. “[They] aren’t funded properly or properly informed by mental health experts. And there’s no shared decision-making between the students and the administrators, which means that their decisions are not based in empathy.”
Kevin Kee, dean of the faculty of arts at the University of Ottawa and chair of the President’s Advisory Committee on Mental Health and Wellness, says that, of the seven committee members, three are students. “We need to address their concerns and we need their advocacy, and the whole point of the committee is to recommend action,” says Kee. He noted that there is a new student adviser to the provost on mental health, and the school has a new tele-psychiatry program in collaboration with the Royal Ottawa Mental Health Centre.
Another student initiative, U of T’s How Many Lives (HML), was established as a tribute to Carey Davis, an undergraduate student who died by suicide in January 2019. “When something like that happens, the first response is wanting to do something to make the world a better place,” says Marium Vahed, Davis’s best friend and a founding team member of HML. The HML Facebook page and website primarily focus on anonymous testimonials. Vahed says they wanted to give students space to share their own stories, which can get lost in all of the talk of policy changes and alleviating wait times. The experiences range greatly, from the welcome comfort provided by a visit to Trinity College’s chaplain to annoyance at “DIY bath bomb” workshops that were seen by students as a substitute for more evidence-based mental health care.
This kind of student engagement is necessary to move forward, says Henderson. “In the past, we would have a youth advisory panel and maybe put a question to them or let them design the posters,” she says. It is an increasingly outdated model—making the group most affected by decision-making just one minor cog in the machine. “Young people must be given the same decision-making power at the table as other people,” says Henderson. “We’re seeing that their lived expertise is as valuable as the technical expertise of the clinician or evaluator.” She recommends engaging young people to actively help with creating new models of care, including which programs are important, how to deliver services and even hiring considerations.
Student-centred steps taken at some institutions have been encouraging. U of T’s task force on student mental health included consultation that involved “listening sessions,” where students were encouraged to share their concerns. Bowman says the report was the most positive step forward he saw during his time at U of T. Brock University has introduced a number of different measures over the past several years, including a workshop that explains anxiety and strategies to manage it; more than 1,400 students have participated thus far. A panel of undergraduate and graduate students advises Brock’s Student Wellness and Accessibility Centre. And the university partners with local agencies, such as Community Addiction Services of Niagara, to help integrate mental health services both on campus and off.
“It’s been very important that we’ve had our Brock Students’ Union and Graduate Students’ Association at the table,” says Anna Lathrop, the school’s vice-provost and associate vice-president. “We’ve had amazing student leaders in governance. They have very much been both advocates and supports.”
Targeted interventions have also made a difference. Memorial University now offers a Stepped Care 2.0 resource, which was developed by the university in collaboration with MHCC and the province of Newfoundland and Labrador. According to the MHCC, focusing on “rapid-access, single-session clinics, recovery-oriented treatment principles and e-mental health programming” has greatly reduced wait times. McMaster University offers an online system for self-reported absences, giving students the opportunity to extend a deadline or reschedule an exam by 48 hours once per term with no mandatory documentation—something many student advocates have linked to stress reduction.
In addition to centralized changes, there have also been diffuse efforts to fill perceived gaps in services. During the December exam period at U of T, “Mindful Moments” sessions were on offer. In January, across dozens of separate U of T-affiliated websites, there were references to guided nature walks and lunch & learns. And as the COVID-19 crisis deepened and buildings across campus closed, some health services remained available, with counselling appointments being offered by phone or video-conferencing.

Institutions are increasingly turning to virtual or telehealth options in a bid to reduce wait times and increase accessibility. U of T recently rolled out My SSP (short for My Student Support Program), a new text and chat helpline service for students that offers free counselling in dozens of languages—particularly important to an institution with a large proportion of international students. UBC also offers thousands of counselling appointments through an online and telephone service called Empower Me, which provides options for in-person, phone, video and e-counselling services in multiple languages, even on evenings and weekends, to UBC students anywhere in North America. It also offers 24-7 access to crisis counsellors.
Some students are also encouraging their institutions to view mental health through an intersectional lens, to broaden their response beyond exams-related stress and encompass a more structural approach that considers the impacts of racism, sexual abuse and poverty.
“The university likes to depoliticize mental health and make it more of a wellness issue,” says Laura O’Connor, a fourth-year political science student at the University of Ottawa and an executive member of the uO Collective. “They will bring in puppy dogs but they won’t talk about class privilege or the financial burden many students take on. They won’t talk about the lack of POC [people of colour] representation in the faculty and how inaccessible so many physical places are. There’s no acknowledgement of how they contribute to forms of oppression we know are linked to mental illness and general distress.”
Kee says that the school recognizes these issues as both urgent and valid. “I am in agreement about the intersectionality of mental health,” he says, adding that he has met with the uO Collective on multiple occasions. “[But] the university is doing quite a lot . . . and we are very aware that different students have different needs.” According to Kee, the University of Ottawa recently hired new mental health staff members “who are sensitive to cultural realities.”
The MHCC’s Mantler says that it’s essential to address the “whole student” when considering mental health supports. “The pandemic has further revealed cracks in the system,” he says. “It’s urgent that students at risk are supported. They are managing everything from unsafe jobs to at-risk living conditions, and it’s important to create services for those facing additional challenges and barriers. We have to ask who needs extra attention, who might need help finding secure housing, including new Canadians, Indigenous students, LGBTQ2+ students, racialized students and international students.”
But addressing the needs of students cannot be done in a vacuum, says Henderson. “No one university is going to be able to tackle this problem on their own. We have to think about how mental health services on campus are funded, what are the appropriate services, how are they designed and how are those services interconnected with the broader community of services that exist.”
In speaking about her friend, Vahed wasn’t simply devastated by personal loss; she was also unsettled by the loss of Davis’s potential. “My friend who died was the most driven of all of us,” she says. “We lost her and we also lost everything she was going to do for the world.”
The university experience is very much a chrysalis. Students typically arrive as adolescents and leave as adults, and along the way they undertake the complex process of better understanding both their identity and place in the world. To facilitate that process, Henderson says that institutions need to ensure that they’re laying the right groundwork. “[Students’] early mental health service experiences will affect what they believe they deserve down the road,” she says. “We’re signalling to young people whether or not this is a system they can count on when they need it, or a system that’s going to be harmful.”
*Name changed to protect privacy
Correction: A previous version of this article mistakenly referred to Joanna Henderson as a psychiatrist. Henderson is a psychologist at the Centre for Addiction and Mental Health.
I’m a contributing editor to Maclean’s magazine, and a freelance features writer for the BBC, Harper’s, ELLE, Cosmopolitan, Vogue, The Guardian, Marie Claire, New York Magazine, Afar, The Walrus, Chatelaine, Globe and Mail, Reader’s Digest, and more. In 2023, I wrote the most-read story in Toronto Life magazine, and two of the top 10 most read stories in Maclean’s magazine. I also host and produce podcasts, including iHeart Radio’s Unrestorable, which peaked at #5 in all Apple Podcasts.
Related Posts

Best Programs By Reputation
My Classroom Will Be AI-Free This Fall
AI Is Ruining My Education

MBA Directory 2025
Subscribe to Message Board, our weekly newsletter guide to planning your post-secondary journey
Whether you’re a student, parent or guidance counsellor, Message Board is a resource you won’t want to miss out on.